|
Overview
 Flat feet are a usually painless condition where the arches on the inside of your feet are completely collapsed arches so that the entire sole of your feet touch the floor when standing. Flat feet can develop after an injury to the foot, such as a ligament, tendon or muscle tear, or as a result of arthritis or they may develop because the condition runs in the family. People with flat feet often complain of their feet rolling inwards when walking or a feeling of their foot collapsing. Causes Genetic predisposition. Faulty foot mechanics, e.g. excessive pronation. Abnormal bony architecture. Laxity of ligaments. Neuro-muscular disease. Trauma to the leg muscles or major tendons. Inflammatory diseases of the joints e.g. Rheumatoid arthritis. Surgical procedures on the leg and ankle. Limb length inequality. Tight Achilles tendon. Symptoms People will have a very heavily dropped arch and it won?t affect them at all and people will have it slightly dropped and it could cause fierce problems. It could cause things like plantar fasciitis, it could cause heel spurs, desperate ball-of-the-foot pressure, or pressure on the big toe known as the hallux which causes discomfort in the foot. It will create problems upwards to the knees, hips and the back once you?re out of line. Diagnosis Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis. pes planus radiology Non Surgical Treatment When pain results from a fallen arch, the physician may prescribe these. Rest and ice. A brace to help support the fallen arch. Physical therapy to strengthen and stretch the foot. Orthotics (arch supports) to compensate for a fallen arch. The physician may tell the patient to choose shoes that have proper arch supports and avoid non-supportive shoes such as flip-flops. If obesity contributed to the fallen arch, the patient should lose weight. Surgical Treatment  This is rare and usually only offered if patients have significant abnormalities in their bones or muscles. Treatments include joint fusion, reshaping the bones in the foot, and occasionally moving around tendons in the foot to help balance out the stresses (called tendon transfer). Flat feet and fallen arches are common conditions that are in most cases asymptomatic. However, in patients who do have symptoms, treatments are available that can help reduce pain and promote efficient movement. Orthotic devices are well recognised as an excellent treatment and podiatrists can offer these different treatment modalities as individualised treatments for patients. After Care Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
0 Comments
Overview
Approximately 75% of us present with one leg longer than the other. It?s staggering, literally, that so many people walk about with an imbalance. Yet to have one leg longer than the other doesn?t seem to create pain for everyone but for those that it does it brings pain in a myriad of dysfunction from TMJ, headaches, low back pain, IBS, bladder problems, sexual dysfunction, sacroiliac joint pain, pubis dysfunction, groin strain, gluteal dysfunction as well as the formation of trigger points. 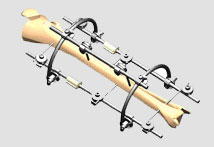 Causes Some children are born with absence or underdeveloped bones in the lower limbs e.g., congenital hemimelia. Others have a condition called hemihypertrophy that causes one side of the body to grow faster than the other. Sometimes, increased blood flow to one limb (as in a hemangioma or blood vessel tumor) stimulates growth to the limb. In other cases, injury or infection involving the epiphyseal plate (growth plate) of the femur or tibia inhibits or stops altogether the growth of the bone. Fractures healing in an overlapped position, even if the epiphyseal plate is not involved, can also cause limb length discrepancy. Neuromuscular problems like polio can also cause profound discrepancies, but thankfully, uncommon. Lastly, Wilms? tumor of the kidney in a child can cause hypertrophy of the lower limb on the same side. It is therefore important in a young child with hemihypertrophy to have an abdominal ultrasound exam done to rule out Wilms? tumor. It is important to distinguish true leg length discrepancy from apparent leg length discrepancy. Apparent discrepancy is due to an instability of the hip, that allows the proximal femur to migrate proximally, or due to an adduction or abduction contracture of the hip that causes pelvic obliquity, so that one hip is higher than the other. When the patient stands, it gives the impression of leg length discrepancy, when the problem is actually in the hip. Symptoms In addition to the distinctive walk of a person with leg length discrepancy, over time, other deformities may be noted, which help compensate for the condition. Toe walking on the short side to decrease the swaying during gait. The foot will supinate (high arch) on the shorter side. The foot will pronate (flattening of the arch) on the longer side. Excessive pronation leads to hypermobility and instability, resulting in metatarsus primus varus and associated unilateral juvenile hallux valgus (bunion) deformity. Diagnosis Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis. Non Surgical Treatment The key to treatment of LLD in a child is to predict what the discrepancy is at maturity. If it is predicted to be less than 2 cm., no treatment is needed. Limb length discrepancies of up to 2 or 2.5 cm. can be compensated very well with a lift in the shoe. Beyond 2.5 cm., it becomes increasingly difficult to compensate with a left in the insole. Building up the shoe becomes uncosmetic and cumbersome, and some other way of compensating for the discrepancy becomes necessary. The treatment of LLD is long-term treatment, and involves the physician and patient?s family working together as a team. The family needs to weigh the various options available. If leg lengthening is decided on, the family needs to understand the commitment necessary to see it through. The treatment takes 6 months to a year for completion, and complications can happen. But when it works, the results are gratifying.  leg length discrepancy test Surgical Treatment Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate. Overview
 Heel pain is one of the most common conditions treated by podiatrists. It is often a message from the body that something is in need of medical attention. Pain that occurs right after an injury or early in an illness may play a protective role, often warning us about the damage we have suffered. The greatest incidence of heel pain is seen in middle-aged men and women. It is also seen in those who take part in regular sporting activities and those significantly overweight and on their feet a lot. Heel pain can also occur in children, usually between 8 and 13, as they become increasingly active in sporting activities. Causes some heel pain can be caused by rheumatological diseases, and these pains can do a real good impersonation of plantar fasciitis symptoms. Seronegative Arthropathies such as Psoriatic Arthritis, Reactive Arthritis and Ankylosing Spondylisis are the most common types to cause heel pain by producing an inflammatory reaction where the fascia attaches to the heel. This is called an enthesitis. If you have a history of Psoriasis or a family history of other arthritic conditions listed above we recommend you see a clinician about your heel pain to confirm the diagnosis. Another occasional cause of heel pain is loss of the cushioning fat pad of the heel, which can result in a bruised heel bone (calcaneus). If you can easily feel your heel bone through your skin on the bottom of your foot you may well have poor fatty tissue on your heel. Pressing on the centre of your heel should feel like pushing into firm rubber, and your skin should not move easily. If you can pinch the skin under your heel and feel a very hard lump when you press the bottom of your heel then it is likely you have a heel fat pad problem. One simple final test is to walk on a hard floor. If you feel the pain only when your heel hits the ground a fat pad problem is most likely. If the pain mainly occurs as you lift the heel off the ground it is more likely to be plantar fasciitis. Symptoms See your doctor as soon as possible if you experience severe pain accompanied by swelling near your heel. There is numbness or tingling in the heel, as well as pain and fever. There is pain in your heel as well as fever. You are unable to walk normally. You cannot bend your foot downwards. You cannot stand with the backs of the feet raised (you cannot rise onto your toes). You should arrange to see a doctor if the heel pain has persisted for more than one week. There is still heel pain when you are not standing or walking. Diagnosis A biomechanical exam by your podiatrist will help reveal these abnormalities and in turn resolve the cause of plantar fasciitis. By addressing this cause, the patient can be offered a podiatric long-term solution to his problem. Non Surgical Treatment Treatment for plantar fasciitis - the vast majority of patients recover with conservative treatments (designed to avoid radical medical therapeutic measures or operative procedures) within months. Heel with ice-pack. Home care such as rest, ice-pack use, proper-fitting footwear and foot supports are often enough to ease heel pain. Non-steroidal anti-inflammatory drugs (NSAIDs) - medications with analgesic (pain reducing), antipyretic (fever reducing) effects. In higher doses they also have anti-inflammatory effects, they reduce inflammation (swelling). Non-steroidal distinguishes NSAIDs from other drugs which contain steroids, which are also anti-inflammatory. NSAIDs are non-narcotic (they do not induce stupor). For patients with plantar fasciitis they may help with pain and inflammation. Corticosteroids, a corticosteroid solution is applied over the affected area on the skin; an electric current is used to help absorption. Alternatively, the doctor may decide to inject the medication. However, multiple injections may result in a weakened plantar fascia, significantly increasing the risk of rupture and shrinkage of the fat pad covering the heel bone. Some doctors may use ultrasound to help them make sure they have injected in the right place Corticosteroids are usually recommended when NSAIDs have not helped. Physical therapy, a qualified/specialized physical therapist (UK: physiotherapist) can teach the patient exercises which stretch the plantar fascia and Achilles tendon, as well as strengthening the lower leg muscles, resulting in better stabilization of the ankle and heel. The patient may also be taught how to apply athletic taping, which gives the bottom of the foot better support. Night splints, the splint is fitted to the calf and foot; the patient keeps it on during sleep. Overnight the plantar fascia and Achilles tendon are held in a lengthened position; this stretches them. Orthotics, insoles and orthotics (assistive devices) can be useful to correct foot faults, as well as cushioning and cradling the arch during the healing process. Extracorporeal shock wave therapy, sound waves are aimed at the affected area to encourage and stimulate healing. This type of therapy is only recommended for chronic (long-term) cases, which have not responded to conservative therapy. Surgical Treatment Only a relatively few cases of heel pain require surgery. If required, surgery is usually for the removal of a spur, but also may involve release of the plantar fascia, removal of a bursa, or a removal of a neuroma or other soft-tissue growth. no foot pain Prevention  Wear shoes that fit well, front, back and sides and have shock-absorbent soles, rigid uppers and supportive heel counters. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm-up before running or walking, and do some stretching exercises afterward. Pace yourself when you participate in athletic activities. If overweight, try non weight-bearing activities such as swimming or cycling. Your podiatrist may also use taping or strapping to provide extra support for your foot. Orthoses (shoe inserts) specifically made to suit your needs may be also be prescribed. |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
July 2017
Categories |
 RSS Feed
RSS Feed
